


Transverse Upper Gracilis Flap (TUG)
The transverse upper gracilis flap utilizes the skin, fat and muscle from the inner thigh. This flap relies on the blood vessels that penetrate the gracilis muscle. The scar resides in the groin just under the bikini line of the inner, upper thigh.
1. Overview
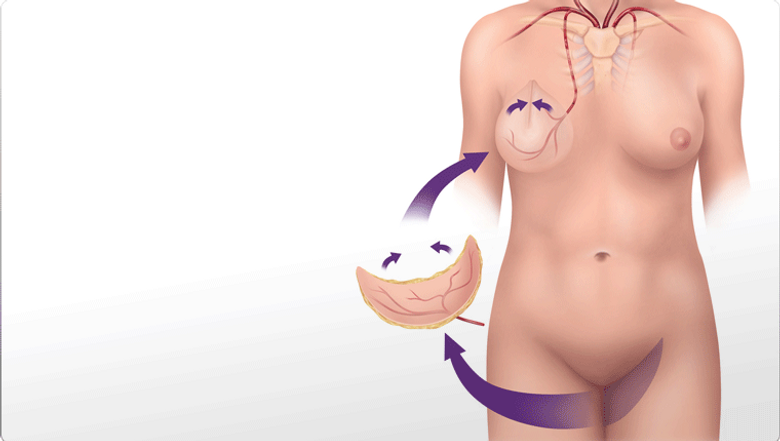
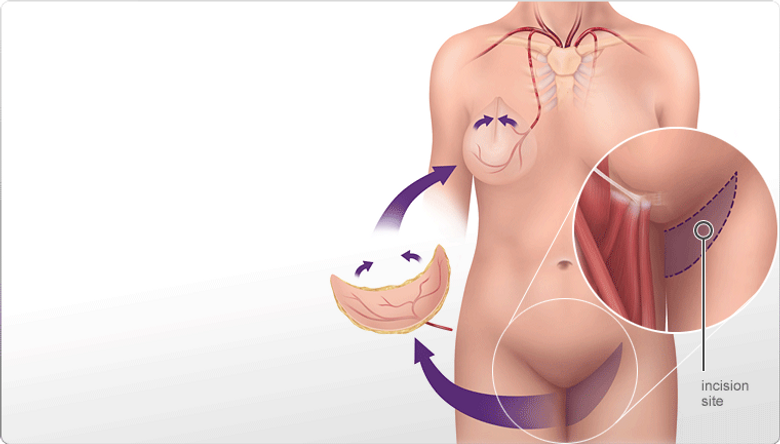
During the procedure, an elliptical portion of skin and fat from the inner thigh is dissected away from all other tissue. The gracilis muscle is also taken with this flap. Dissection then proceeds towards the medial circumflex artery which is used to give the flap blood flow.

The flap is then transferred to the chest wall. The vessels that supply blood to the flap are sewn to the internal mammary artery and vein which lie under the ribs next to the sternum. A small (3cm) portion of the third rib costal cartilage is removed to reveal the underlying vessels. A microscope is used to help the surgeon visualize the vessels so that they can be sewn together.

2. Preoperative Considerations
The typical candidate for the TUG flap surgery is a thin woman with insufficient abdominal tissue for the DIEP flap and insufficient buttock tissue for the SGAP flap.
Patients that are not candidates for this type of surgery include:
Patients that smoke
Patients that are professional athletes
Patients with a BMI > 32. Click here to calculate your BMI.

One-sided surgery:
This surgery takes 4 hours. Drains are required in the breast as well as the inner thigh and these are usually removed on post-operative day 10.
Two-sided surgery:
This surgery takes 8 hours. Drains are required in the breast as well as the inner thigh and these are usually removed on post-operative day 10.
3. Surgical Considerations

Patients stay in hospital for 3-5 days and require frequent checks of the flap by the ward nurses to evaluate blood flow. Patients must lie flat for the first two days after surgery to decrease the tension on the incision on the thigh. Flexion of the hips is minimized for the first two weeks following surgery.
Patients are unable to drink caffeine for one month after the surgery and must take aspirin once per day for a month.
Following surgery patients are restricted from exercise or heavy activity for a period of 4 weeks. Patients typically return to work after 4 weeks. Nipple reconstruction is performed 3 months following flap surgery.
4. Postoperative Considerations

Wound healing complications (20%)
Mastectomy flap necrosis (15%)
Seroma (15%)
Fat necrosis (10%)
Scar visible below bikini line (common)
Widened scar (common)
Hematoma (5%)
Total flap failure due to a blood clot (1-2%)
Infection (1-2%)
Hypertrophic scarring (0.5%)
DVT (0.07%-3.5%)
PE (0.09%-2%)